
In a multitude of instances, parents have been kept in the dark about schools socially transitioning their children. These instances, which I have only sampled, are from across the country and stem from fundamental beliefs held by many teachers, guidance counselors, administrators, and policymakers that they know better than parents how to provide for children, especially on the transgender issue. They believe that affirmative care is the only acceptable option for students claiming a transgender identity and that even the possibility of parental refusal of such care is an unspeakable evil. They believe that parents who don’t affirm transgender identities need to be prevented from interference, and school policies around the country reflect that view.
In my previous article, whosechildren I examined Virginia Department of Education and Fairfax County Public Schools policy around school involvement in the care of children who assert transgender identities and made a primarily legal argument for why those policies are bad1. This article will focus on why parents might not want to provide affirmative care and why accusing parents of child abuse if they refuse to affirm a transgender identity is incorrect.
What is “Gender-Affirming” Care?
Affirmative care takes on three increasingly permanent forms: social transition, hormone therapy, and “gender-affirming” surgery. The stated goal of such care is to improve health outcomes for people who identify as transgender. In the past it was sometimes prescribed to adults who exhibited gender dysphoria which is a condition entailing distress over one’s gender. Recently children have begun to exhibit similar a condition described by the DSM-5, in part, as: “A strong desire to be of the other gender or an insistence that one is the other gender2.” However, gender dysphoria is not viewed as a requirement for transgender status by some. In VDOE promoted so-called best practices for school counselors, transgender is defined as “an umbrella term used to describe those who challenge social gender norms, including genderqueer people, gender-nonconforming people, transsexuals, crossdressers, and so on” which is only applicable if self-applied. Such a definition underlines the fact that desires to transition are not always driven by distress at one’s gender3 and that the word has a very broad meaning4. As such, when a child asserts that he or she is transgender and needs to transition parents, doctors, and mental health professionals need to identify why a child has identified as transgender and not support transition as the default course of action.
What is Social Transition?
The first step in affirmative care is social transition, a set of changes which typically involve the use of pronouns that differ from the sex observed at birth and a change of name to one that more closely maps to the person’s identified gender. Though it does not involve medical treatments, it can involve practices that conform the body more closely to one typical of the opposite sex, eg: breast binding, a practice which has a “nearly universal negative physical impact.” Social transition is associated with persistence of gender dysphoria, a condition that has historically resolved itself for large majorities of children who presented with symptoms. Social transition is not necessarily related to improved social well-being and, according to psychotherapist Lisa Marchiano:
“It appears likely that being conditioned to believe you are the opposite sex creates ever-greater pressure to continue to present in this way, especially in young children.”
Social transition starts, and contributes to, a snowball effect that leads to increasingly invasive medical treatments[^5].
What are Puberty Blockers?
The next step of affirmative care for children is the application of puberty blockers. These drugs stop the natural progression of puberty in children by suppressing the hormones that trigger it. Like social transition, application of puberty blockers is associated with persistence and continued medicalization, and while the effects of puberty blockers on persistence are relatively clear, their purpose is not. The judgement in Bell v. Tavistock, a court case in the UK that dealt with the Tavistock clinic’s prescription of puberty blockers, explains the opaque nature of puberty blockers clinical use:
“There is a lack of clarity over the purpose of the treatment: in particular, whether it provides a “pause to think” in a “hormone neutral” state or is a treatment to limit the effects of puberty, and thus [creates] the need for greater surgical and chemical intervention later”
Further, information on the long-term effects of puberty blockers when used as treatment for gender dysphoria leaves much to be desired. What we do know is that those treated with puberty blockers have relatively lower bone density in comparison to populations that were not treated with the blockers, and, in one study, “left up to a third of patients with abnormally low bone density.” This is unsurprising because bone mass increases rapidly during puberty and advocates claim that bone density recovers once puberty is resumed, either on artificial cross-sex hormones or naturally. However, some evidence indicates that, though bone density increases during the application of cross-sex hormones, those who are treated with cross-sex hormones still have lower bone density than others of the same age and sex observed at birth. There is also extremely limited knowledge on the effects of puberty blockers on brain development and other factors.
Varied effects have been found regarding mental health outcomes for those undergoing puberty suppression, some positive and some negative, but the studies on the subject are all of low statistical power. A comprehensive review of literature on puberty blockers undergone by the National Institute for Health and Care Excellence (NICE) found available evidence on puberty blockers, on all metrics, physical and mental health related, to be of low certainty. The studies were all small, all uncontrolled, and all reviewed studies “reported physical and mental health comorbidities and concomitant treatments very poorly.” Any potential mental health improvements shown in the studies could have been the result of psychological treatments rather than the blockers themselves.
Forgetting for a moment the lack of solid evidence relating to the usefulness of puberty blockers, even their purpose is unclear and obfuscated.
What is Hormone Replacement Therapy?
Hormone replacement therapy, or HRT, is the next step on the “gender-affirming” pathway of medical treatments. These treatments administer hormones to change secondary sex characteristics and create physical and mental changes that more closely match the identified gender. Those observed female at birth (OFAB) take testosterone and those observed male at birth (OMAB) take estrogen. Unsurprisingly, HRT is correlated with persistence. Where puberty blockers are partially reversible depending on when and how they are administered, HRT creates irreversible physical changes in its recipients.
The effects of HRT vary drastically depending on which hormones are administered but one shared side effect is significant damage to fertility. Those who are prescribed testosterone have increased facial hair growth, a lowered voice, and may stop menstruating. They also have significantly higher rates of heart attacks and strokes compared to people of both sexes not on hormones. Prescriptions of estrogen also lead to vocal changes, as well as breast development, decreased facial hair growth, and changes in mood. Those taking estrogen face increased likelihood of heart attacks and, if previously on puberty blockers, lower bone density. Mental health does appear to have at least short-term improvement after administration of HRT, though the effect seems to vary by sex. In its evidence review on pediatric applications of HRT, NICE found the available studies on the subject to be of very low certainty and concluded that:
“Any potential benefits of gender-affirming hormones must be weighed against the largely unknown long-term safety profile of these treatments in children and adolescents with gender dysphoria.”
Other evidence reviews have come to similar conclusions. The use of HRT, especially when it comes to children, is not settled science.
What is Sex Reassignment Surgery?
The final stage of affirmative care, which is generally not administered to minors5, is sex reassignment surgery sometimes known as “gender affirmation surgery.” It goes without saying that these surgeries are not reversible6. OFAB individuals primarily receive double mastectomies and much rarer cases other surgeries like phalloplasty and metoidioplasty7. OMAB individuals often opt for breast augmentation and sometimes feminizing genitoplasties or orchiectomy. These surgeries have risks and are not undertaken by all transgender people. Studies have found mixed results on the long-term effects on mental health for sex change surgeries, but they appear to have positive effects for some who have gender dysphoria, even if overall quality of life does not always improve as a result of the surgery. When it comes to children, it seems that, with possible extreme exceptions, these surgeries, except for mastectomy, are not undertaken, and, according to the Society for Evidence Based Gender Medicine (speaking regarding the aforementioned mastectomies),
“The current state of scientific knowledge does not support the assertion that “gender-affirming” surgical interventions for minors are safe, effective, and medically necessary.”
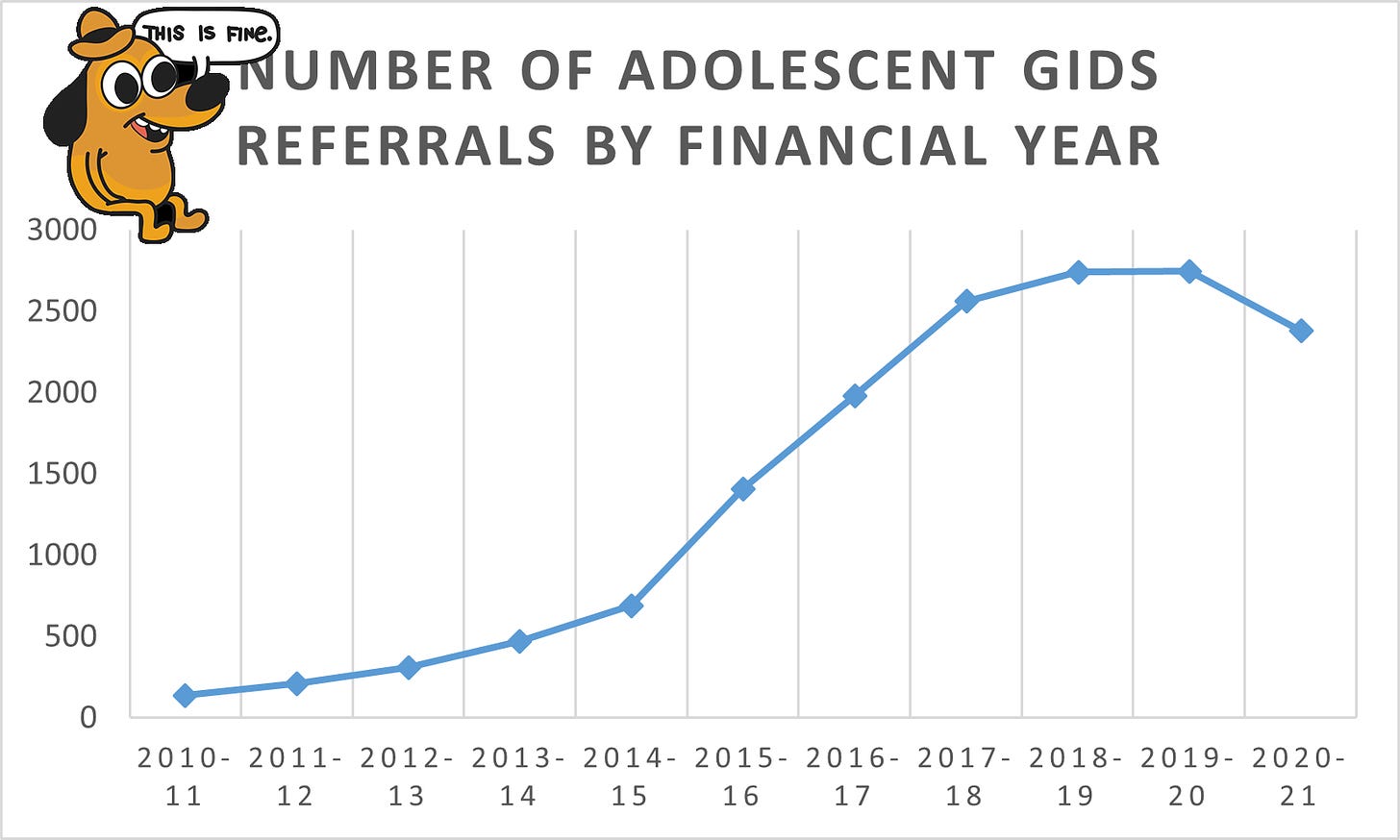
GIDS stands for the Gender Identity Development Service, and referrals are to the UK’s only gender clinic
For all interventions, social, medical, and hormonal, the evidence for efficacy is very weak and studies lack information on long-term effects of treatment. Exacerbating the dearth of data even more is the fact that “currently, [gender dysphoria] predominantly presents in adolescent females with no childhood history” a patient group with even less evidence of treatment efficacy than “prior predominantly male and childhood-onset [gender dysphoria] presentation.” We are in uncharted waters when it comes not only to the sheer amount of youth identifying as transgender, but also with the sex of those who identify as such. In the past primarily boys were diagnosed with gender dysphoria, but in the past decennium8 a huge spike in girls identifying as transgender has occurred, a vast demographic shift.
What is Exploratory Psychotherapy?
“Gender-affirming” care is not the only treatment option; exploratory psychotherapy is a working alternative9 to “gender-affirming” care and is significantly less invasive than its alternative. This treatment seeks to understand the root cause of gender dysphoria and determine the most useful and ethical treatments based on the results. Exploratory psychotherapy proposes that parents
“Listen to whatever your child has to say on the subject [of gender] if they bring it up, be interested, but make no contribution of your own and never initiate [a conversation on gender].”
In short, allow children to develop their identities, without significant interference, and allow them to act outside of traditional sex-based roles without suggesting to the child that doing so means they were born in the wrong body10. This approach, assisted by a psychotherapist, does not result in abnormally low bone density, nor does it cause permanent damage to fertility.
Conclusions and Child Abuse
All of this information, especially the existence of the stepping stones of persistence (social transition ➡ puberty blockers ➡ cross-sex hormones ➡ sex-change surgery), is important for parents to understand if they are to make informed decisions about their child’s health. Given the lack of solid evidence for gender affirmative treatments, it should go without saying that choosing to follow a path other than direct affirmation, especially with limited to no psychiatric intervention and investigation, is not child abuse, but, given relatively recent court cases in Texas and California, it’s worth spelling out the argument.
Is Denying “Gender-Affirming” Child Abuse?
An abused or neglected child is defined in § 63.2-100 of the Code of Virginia as a child
“Whose parents or other person responsible for his care creates or inflicts, threatens to create or inflict, or allows to be created or inflicted upon such child a physical or mental injury by other than accidental means, or creates a substantial risk of death, disfigurement, or impairment of bodily or mental functions” or “whose parents or other person responsible for his care neglects or refuses to provide care necessary for his health.”
I hope, by this point I’ve shown that there is currently not enough evidence to prove that “gender-affirming” care is necessary for the health of children.
To go further, parents who believe that their child will grow up to be healthy and happy in their own body without medical interventions or surgery, if that identity isn’t affirmed in the present, might even feel that affirmation itself would be abusive. After all, medical procedures of that variety cause substantial risk of impairment to bodily functions like fertility, and most surgeries guarantee loss of such functions11. Even regretted social transitions can cause lasting distress. This isn’t to say that “gender-affirming” care is necessarily abusive, and terrified parents, scared into believing the false “transition or die” narrative can hardly be blamed12 for placing their trust in doctors and therapists who ought to be giving their children evidence-based treatment.
However, it seems very likely that many people who are undergoing these treatment would have desisted were a different path taken, a likelihood only exacerbated by the rise of care models that overlook the importance of psychological assessments (in youth especially, significant psychiatric comorbidities are often present along with gender dysphoria). Not only that, but the stories of the growing13 detrans movement suggests that, for those who change their mind after surgery and hormones, regret can be immense, and desistance carries its own burdens14.
The Conclusion
If I were the parent of a child claiming a transgender identification, I would not leap to provide affirmative care: social transition, puberty blockers, and/or hormones. Instead, I would run screaming, to the hills15 if necessary. It is my finding that, given the poorly studied risks and benefits of affirmative treatments, the best, and safest course for children displaying gender dysphoria and identifying as transgender is exploratory psychotherapy, especially given the likelihood that many currently presenting cases of gender dysphoria may be spread by social contagion.
Social transition shows mixed results. Puberty blockers and HRT are both experimental treatments that broadly use drugs off-label. Sex-change surgeries are irreversible. Across the globe, medical organizations are taking increasingly cautious stances on pediatric transition. Parents need to be able to make informed choices about the care of their children, and schools need to step out of the way.
Footnotes
-
Looking back on it, it might have been better for everyone if I had stuck with my original plan and merged these two articles ↩
-
The full criteria is longer but this is the primary criterion ↩
-
The term gender euphoria is notable in this equation, as well as the general awkwardness of growing up.
“Suzie, just because you’re uncomfortable in your own body, that doesn’t mean you would be better off as a boy.” ↩
-
These definitions also drive me crazy. I suspect that James Lindsay has started asking the question “What is a transgender person?” because this definition creates a path of circular logic identical to the one raised by the question “What is a woman?” notably asked by Matt Walsh in his documentary of the same name. ↩
-
With the exception of mastectomies ↩
-
Though several policy documents, studies, letters, and statements have made sure to mention the fact just in case anyone got confused ↩
-
Science has gone too far; the spelling of that word is too much for my mind to handle ↩
-
This just means decade, and it was used in a Swedish(?) paper that I saw, and it was such a fun word I had to include it. ↩
-
That is, it is an alternative in states that haven’t banned it under the pretense that a) transgenderism is the same as homosexuality and that b) it is attempting to change gender identity. Such bills reflect the level of ideological capture in legislatures that has occurred in the recent past. ↩
-
At this point, a significant portion of my soul wanted to insert a crudely drawn image of Chuck-E-Cheese saying, “Let kids be kids” and only the small amount of self-respect that I have managed to retain over my 18 years managed to stop me. ↩
-
It feels like every week or so a reddit post crops up from a detransitioner expressing heart-rending regret over a double mastectomy and the loss of the ability to breastfeed. ↩
-
the doctors can be though ↩
-
I had ascendant here originally, but I think this works a lot better (even though ascendant is a fun word!) ↩
-
Were it not for these stories, I probably would have left this article in the planning stage and moved on to research something less painful to the soul. ↩
-
it’s worked for some people (please note, it is recommended to bring the child in this fleeing to the hills) ↩